
Information
Orforglipron vs Ozempic, Mounjaro and Retatrutide

Sep
Although AusAminos.com is primarily focused on peptides, we’re ultimately agnostic regarding GLP-1 agonist delivery mechanisms. Today, we’re talking about a non-peptide GLP-1 agonist called orforglipron, which is notable for its imminent availability and oral small-molecule mechanism of action, allowing it to be taken as a pill rather than by injection.
How does orforglipron compare with Ozempic and Rybelsus?
The best results we’ve seen for orforglipron came from a phase 2 study in September 2023. It ran for 36 weeks and had 45mg (taken daily) as the highest dose – participants weren’t diabetic and had a mean BMI of 37.9. After 36 weeks, the 45mg cohort had a mean bodyweight reduction of 15.4%, although the 24mg cohort – around half the dose – managed 13.6%. Vomiting and nausea were most common in the 24mg cohort, although this is almost certainly due to the quick titration scheduling that they underwent.
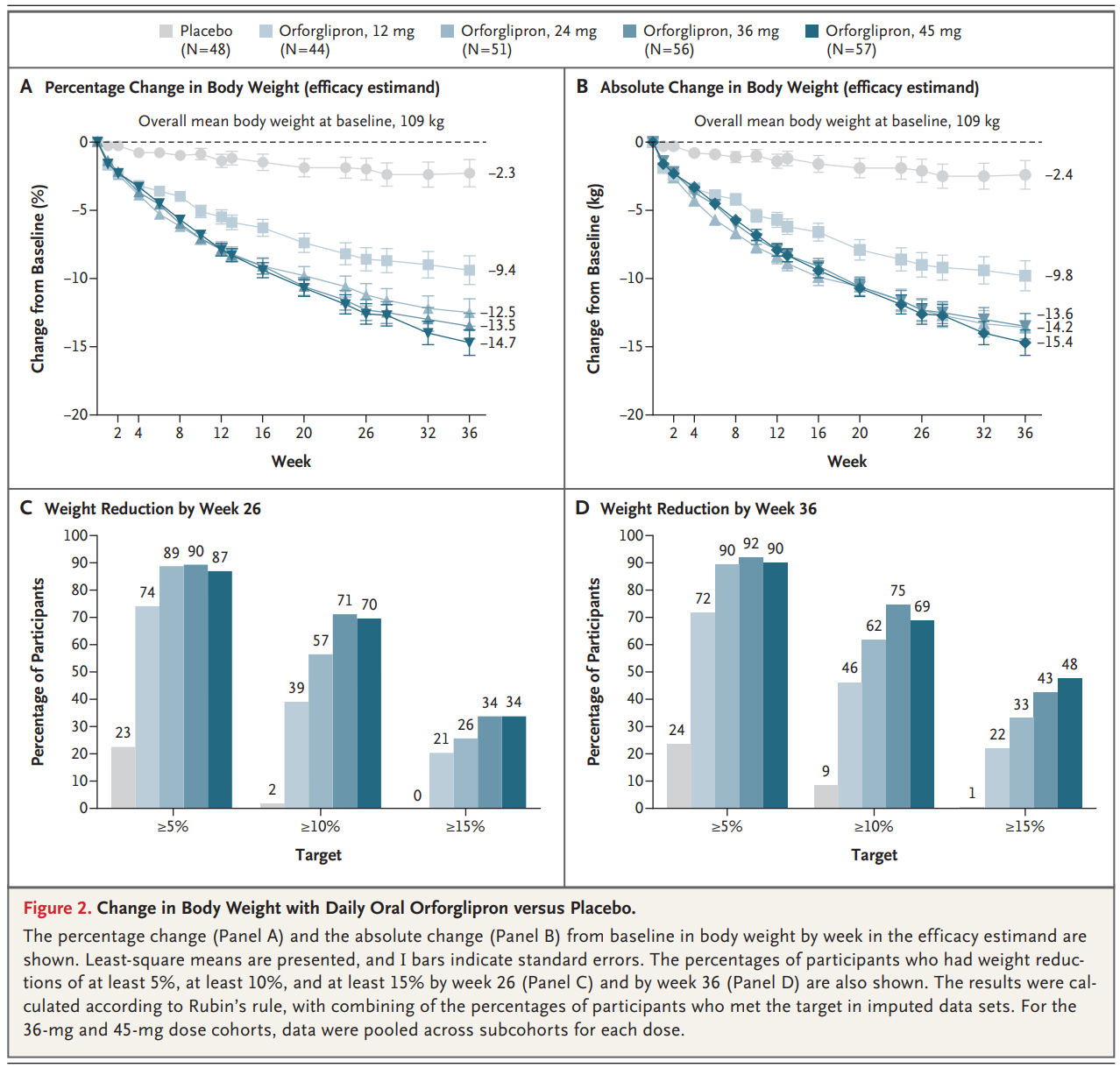
In the biggest phase 3 study that looked at orforglipron stacked up against a placebo in patients with diabetes, weight reduction on the largest dose (36mg) was 7.9% over 40 weeks. Lower doses of 3mg and 12mg showed a 4.7% and 6.1% weight loss reduction over the same time period respectively.
How does semaglutide, the active peptide in Ozempic and Wegovy, compare? From the original STEP-1 phase 3 study, we have the following data on semaglutide:
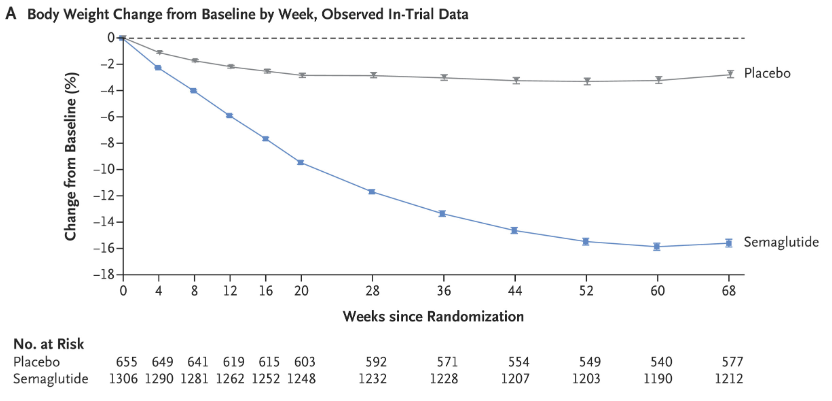
At a dose of 2.4mg per week, semaglutide comes in at around 14% weight reduction at the 40 week mark. The STEP-1 phase 3 study was also in patients without diabetes, and we know from the data that diabetics generally lose about half as much weight on GLP-1 RAs compared to non-diabetics. Looking at the evidence, orforglipron is roughly as effective as max-dose subcutaneous semaglutide injections, even at sub-maximal doses (24mg likely being the sweet spot, albeit with a less aggressive titration schedule).
Oral semaglutide, sold as Rybelsus, resulted in around 15% weight reduction, but this occurred over the course of 68 weeks at the max dose of 50mg per day. Since weight loss hadn’t plateaued in either orforglipron study, I consider orforglipron a superior oral option.
Pros of orforglipron
One of the main benefits is that orforglipron is an oral medication with quite a stable shelf life and relatively low storage precision requirements. Almost all peptide-based GLP-1 RAs are subcutaneous injections, with some having stricter storage and usage requirements (i.e. limited shelf life and must be stored in a refrigerator). Some mobility impaired people might struggle with injections, whereas others might struggle to get over the psychological hurdle of using a needle. Additionally, it’s hypothesized that an easier manufacturing process compared to peptides will make the medicine available at a lower price than rival GLP-1 agonists. Competition tends to bring prices down, and Lilly might come in at a low price point to contest the market share Novo Nordisk still has with semaglutide and in particular, its Rybelsus product (oral semaglutide). Usage restrictions (fasted, time of day, etc.) are also more relaxed than other GLP-1 RA orals.
Cons of orforglipron
At the highest (36mg) dose in ACHIEVE-1, 8% of trial participants discontinued usage owing to adverse events, with vomiting and nausea reported in 14% and 16% of participants respectively. Oral GLP-1s tend to come with more side effects, and because gastrointestinal uptake is lower than with subcutaneous injections, a higher dose is required (which increases costs). For reference, the rate of discontinuation in the semaglutide study referenced above was 4.5% – around half the rate of orforglipron with a longer trial period. It’s also not known if the cardioprotective aspects of GLP-1 agonists will be the same with users of orforglipron, and it may take quite some time until that data is available.
The verdict
Orforglipron is about as effective as subcutaneous semaglutide injections but has more side effects. If injections are acceptable, Mounjaro (tirzepatide) outperforms both for weight loss. If needles are off the table, orforglipron will be the best oral GLP-1 RA option.
Best guess availability: US late 2026; Australia mid-2027.